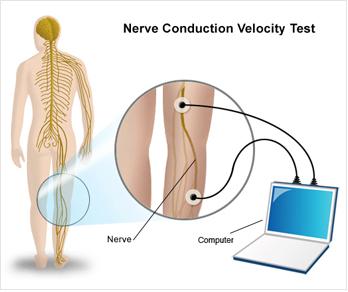
Nerve Conduction Velocity (NCV) is used to measure action potentials resulting from peripheral nerve stimulation. The reaction times (latencies) and velocities obtained will detect neurological problems or compression of the nerves throughout the extremity.
The F-Wave looks at the most proximal segment of the nerve, including the root. The reaction time (latency) will show if there is a delay at the spinal level of the particular nerve.
The Tibial H-Reflex is considered to reflect that state of the S1 nerve root and its sensory component.
Collectively, the F-Wave and H-Reflex look at compression at the cord level.
By testing both the motor and sensory components of the nerve, a doctor can obtain a comprehensive picture of the patient’s problem areas.
“The clinical utility of Nerve Conduction Velocities (NCV) is based upon its ability to: 1) demonstrate abnormal sensory function when the history and/or neurological examination are equivocal; 2) reveal the presence of clinically unsuspected malfunction in a sensory system, when demyelinating disease is suspected because of symptoms and/or signs in another area of the Central nervous System (CNS); 3) help define the anatomic distribution of a disease process; and 4) monitor objective changes in a patient’s status.
These tests provide reproducible, sensitive, quantitative extensions of the clinical neurological examination…NCV’s are essential to the modern practice of medicine because they: 1) provide data unobtainable without the use of amplifiers and oscilloscopes; 2) quantify and objectify data which the clinician may sense; 3) localize lesions within a long sensory pathway; 4) are more efficient and cost-effective because the testing is done by paramedical personnel who can be trained more expeditiously than neurologists, ophthalmologists and otolaryngologists.”
- Chiappa, M.D., Evoked Potential in Clinical Medicine, (condensed and reprinted).